![]()
![]()
![]()
|
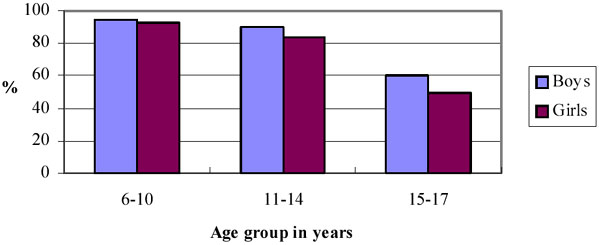
The gender gap in primary education is minimal. |
Total enrolments of school aged children increased in the five year period 1992-93 to 1997-98, resulting in 94 percent of primary school aged children enrolled in school. Children are starting school earlier and staying in school longer, and the gap between girls' and boys' enrolment has declined. Figure 10 shows enrolment rates of girls and boys at different ages, based on 1997-98 data. There now exists very little difference between the enrolment rates of boys and girls of primary school age. However, a significant gender gap is still apparent in the secondary school age group, which increases in the upper secondary school level.
Figure 10: School Enrolment Rates of Boys and Girls by Age Group, 1997-98
|
Girls in urban areas are more likely to attend school than those in rural areas. |
The gender gap in education may be measured by the difference between the proportion of girls and boys enrolled in school. On average, the gap has declined over the five-year period from an 11 percentage point difference to a 6 percentage point difference in lower secondary school ages. In upper secondary school ages the gap has declined from a 15 percentage point difference to an 11 percentage point difference. However, among children of ethnic minority and within the poorest segment of society, there has been very little change. The educational gender gap has actually widened for children of parents with no education. For girls, school attendance is lower in rural areas compared to urban areas. For boys, school attendance is similar across both areas. This implies that boys attend school regardless of residence, whereas, girls in rural areas are more likely not to attend school.
The general increase in primary school enrolment is due in part to a trend toward early and on-time start of grade one. However, data on grade progression shows that a large percentage, ranging from between 45 and 75 percent, of children, are behind their target grade, that is, the grade in which they should be for their age. More girls are on target (60%) than boys (54%). Although girls perform better than boys and are more likely to be on target than boys, it is boys who are more likely to continue schooling beyond lower secondary school.
|
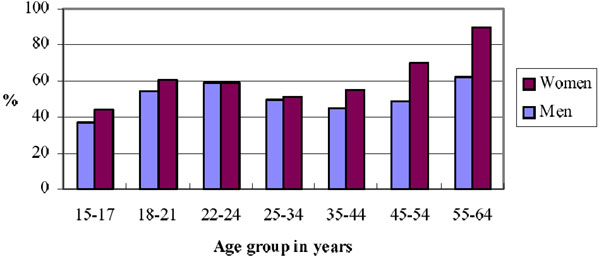
A gender gap in education beyond primary level is re-emerging. |
A disappointing feature of current patterns of educational enrolment and completion is the re-emergence of a gender gap in adult levels of education. Figure 11 shows the proportion of men and women who have completed no more than primary education. It shows that although the gender gap in the share of men and women with primary education has disappeared between those aged 22-24 years, it has re-emerged between those aged 18-21 and 15-17 years, where 6 to 7 percent fewer women than men have advanced beyond primary education. This discrepancy represents a significant efficiency loss to the educational system in general, as girls tend to perform better in school than boys in maintaining their target grades.
Figure 11: Proportion of Men and Women with No More Than Primary Education, by Age Group, 1997-98
|
Women are less well nourished than men. |
Both adult men and women reported improvements in their nutritional status between 1992-93 and 1997-98, with the improvement being greatest among men. Adult women are still more likely to suffer from chronic energy deficiency than men. The gender gap in adult nutritional status is greatest in rural areas, in poorer households and amongst people of ethnic minority. This suggests that in the most disadvantaged households, women have access to relatively fewer resources than men.
|
Recent improvements in child nutrition hove benefited boys more than girls |
There has been a significant improvement in children's long-term nutritional status over the five-year period. Long-term nutritional status is measured by indicators of stunting (diminished height for age). The proportion of children 10 years of age and younger who exhibit signs of stunting has declined from around 50 percent to 38 percent over this period. However, the improvement was greater for boys than for girls. Forty one percent of all girls under 10 years of age still exhibit signs of stunting, compared to 35 percent of boys. On average, there is no statistically significant gender difference in short-term nutritional status, identified by incidence of wasting of children (diminished weight for age). However, girls in rural areas exhibit significantly higher levels of wasting than girls in urban areas.
|
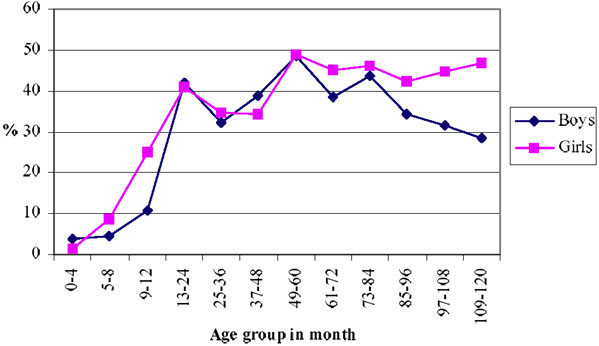
There is some evidence that boys are better nourished than girls. |
Figure 12 shows rates of stunting across age groups, for children up until the age of 10. There is little statistically significant difference in stunting recorded between girls and boys younger than 5 years of age. However, among children 5 to 10 years of age, girls exhibit rates of stunting significantly higher than those of boys.
Figure 12: Moderate to Severe Stunting in Boys and Girls by Age Group, 1997-98
|
Women report illness more than men. |
Rates of reported illness are significantly higher among women than among men. Within a four-week reference period, 44 percent of women aged 18-55 reported illness, compared to 35 percent of men of the same age. Although women report greater incidence of illness than men, they typically return to work sooner than men when having been ill. Both women and men report greater frequency and length of illness in rural areas than in urban areas.
Age is an important contributing factor to illness. Both men and women over the age of 55 reported high incidence of illness; 70 percent of women and 60 percent of men.
|
Women make use of health services more than men. |
Among adults aged 18-55 years, utilisation of health services by women (40 percent of women) is considerably higher than utilisation by men (30 percent of men). Age is again an important factor, with 64 percent of women and 52 percent of men over the age of 55 having consulted a health care practitioner in the four-week period. The higher use of health services by women does not reflect greater use of any one particular type of health service. Approximately three-quarters of both men and women treat themselves with the purchase of medicines from pharmacies without prescriptions.
|
Young boys have illness reported more often than young girls. |
Illness rates of boys younger than 6 years of age are significantly higher than those of girls, as measured by respondents (guardians') self-reporting. This difference is heightened particularly in rural areas. It is not apparent if the gender difference is due to higher rates of reporting of illness, or greater actual illness among boys than girls. Children aged between 6 and 10 exhibit no significant gender differences in rates of reported illness.
|
Boys and girls have equal rates of vaccination. |
Approximately 58 percent of children aged over 12 months are reported to have received the basic set of vaccinations (BCG, DPT, Polio and Tetanus), and there is no gender difference apparent in vaccination rates. However, children born to women with at least primary education report significantly higher rates of vaccination than those born to women with less than primary, or no education.
|
Boys and girls have equal access to health care when reported ill. |
About one-half of all children less than 6 years of age utilised health services in a four-week period. Of those who were ill during this period, 86 percent utilised health services. There is little gender difference in the rate of access to health care, although girls in urban areas have significantly higher rates of contact than girls in rural areas, when ill. Boys also report higher rates of contact in urban areas, but the difference is less.
|
A mother's education impacts on a child's access to health care. |
A mother's level of education has a great impact on access to health care for children, particularly for girls. Only 65 percent of girls under the age of 6 who were ill had accessed a health care practitioner, when their mother had no education. The proportion of ill young girls accessing health care jumps to 88 percent with as little as one to four years of education for the mother. For boys, this impact sees access rise from 74 percent to 91 percent, when ill. A father's level of education has little impact on health care for either girls or boys.
|
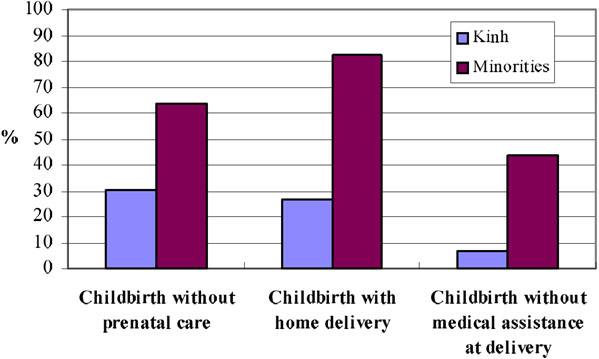
Pre-natal care is low amongst women from disadvantaged households. |
Almost two thirds of all women who are pregnant obtain pre-natal care, though the average number of consultations (1.7) is less than optimal (3), as defined by the Vietnamese Ministry of Health. Use of pre-natal care has increased in the past 5 years, but it still tends to be low among women from poorer households, women of ethnic minority, and women with less than primary education. Eighty one percent of urban women obtain pre-natal care, compared to only 62 percent of rural women.
Figure 13 shows conditions of childbirth by women's ethnicity.
Figure 13: Conditions of Child Birth by Woman's Ethnicity, 1997-98
|
Delivery at home is common. |
Approximately one third (31%) of all women give birth in hospitals. Another third deliver in commune health centres, with the final third delivering at home. Delivery at home is typically more frequent among rural women. Forty-four percent of women in rural areas deliver at home, compared to only 7 percent of urban women. Home delivery is overwhelmingly prevalent amongst women from the poorest households, women of ethnic minority and women with no education.
Doctors assist at 44 percent of all births. Nurses, midwives and traditional birth attendants assist a similar proportion of deliveries. Approximately 30 percent of deliveries on combined average amongst women from the poorest households, women of ethnic minority, and women with no education are unassisted by trained health personnel.
|
IUD use is predominant. Condom use has increased slightly. |
Modern medical contraceptive use is prevalent among married women, with IUDs the most frequently used method. Among married women who have not had any children, contraceptive use is minimal. In urban areas, contraceptive use increases after the first birth and in rural areas it is the second birth that marks a large increase in use. In both rural and urban areas, use of modern contraceptives is significantly higher if one of the first two births results in boys.
In rural areas, 73 percent of married women who use contraception use IUDs. In urban areas, the method mix is more diverse but IUDs still account for 61 percent of all married women who use contraceptives. The share of condoms in the method mix has grown in the past 5 years but still remains minimal at 6%. Traditional methods such as the rhythm method and withdrawal are also popular.
![]()
![]()
![]()
{kind=link}
{kind=link}
{kind=link}
{kind=link}