![]()
![]()
![]()
Planning does not take place at a specific point in time, but rather is a dynamic, ongoing process. The planning process is sometimes referred to as an "iterative" process because it involves the repetition of a series of sequential steps. Assessment of the problem is followed by analysis of its causes, which is followed by development of an action plan, which leads to implementation of the action plan. Assessment or evaluation of the action plan leads to analysis of the reasons for success or failure, development and implementation of modifications to enhance the programme's impact and cost-effectiveness, evaluation of the modified programme, and so on. (See Figure 3.1.)
Many countries have established mechanisms to plan and implement strategies to address micronutrient malnutrition. As a result of commitments made at the World Summit for Children and the International Conference on Nutrition, governments are engaged in developing and implementing national plans of action to improve nutrition, including specific measures to eliminate or substantially reduce deficiencies of vitamin A, iron and iodine. Conducting an assessment, analysis and review of available resources (collectively referred to as "situation analysis") serves as a basis for many national planning efforts to identify and implement micronutrient deficiency prevention strategies.
An analysis of the causes and determinants of micronutrient malnutrition can be undertaken by an existing group that deals with intersectoral nutrition issues or by a new group that is formed specifically to address micronutrient malnutrition issues. Those invited to participate may include representatives of local academic institutions, relevant government bodies, the food industry and non-governmental organizations (NGOs) that implement health and agricultural programmes at the grassroots level.
Figure 3.1. The planning process (adapted from FAO/WHO 1992b)
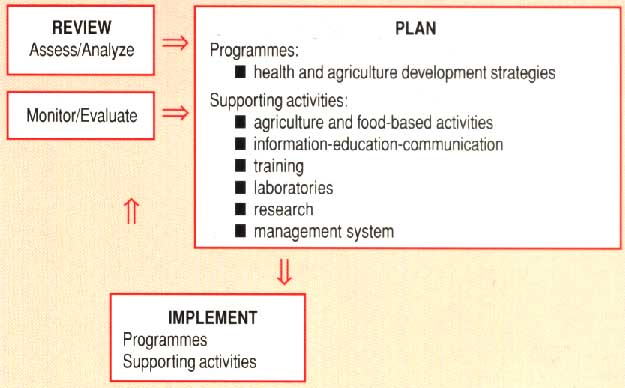
Early in the planning process, a review should be undertaken of the technical and financial resources available to address problems and prevent their recurrence. Such a review will ensure that plans are built on existing infrastructure and activities and will assist in developing or modifying relevant government policies; designing programme strategies and supporting activities such as research and training; and implementing, monitoring and evaluating the resulting integrated programme.
This chapter discusses the range of issues that need to be considered in the process of planning food-based strategies to prevent micronutrient deficiencies.
The first step in assessing the micronutrient status of a population involves determining the prevalence, severity and distribution of micronutrient deficiencies. l his is usually done by using clinical and biochemical indicators of deficiency. Maximum use should be made of existing information, such as reports and data from ministries of agriculture and health, FAO and WHO offices, surveys by NGOs, and the scientific literature. Additional information may be obtained through interviews with relevant local officials and experts. Table 3.1 summarizes the steps in assessing the micronutrient status of a population.
Table 3.1. Steps in Assesing Micronutrient Status
Key Issues/Objectives |
Practical Approaches | |
Initial Assessment |
Is there likely to be a problem with micronutrient deficiency? |
Use existing data from in- country surveys from similar populations. |
Are the problems getting better or worse? |
Conduct rapid assessments in suspected high-risk areas. | |
What areas, populations, age groups are most likely to be at risk? |
||
Review case reports experiences of individuals working in the areas, community-level perceptions of the problem. | ||
What other nutritional and health problems affect the population? |
||
Epidemiological Assessment |
Identify possible underlying causes (inadequate intake, high infection rates, socio-economic and market factors). |
Conduct sample surveys focused on high-risk areas. |
Quantify the severity of the problem on specific at-risk areas/groups. |
Include community level assessments of dietary petterns, seasonality in availability of micronutrient- rich foods, access to markets, agricultural extension, communication channels, health services. | |
Identify potentially effective interventions. |
||
Conduct more detailed dietary assessment, including infant feeding practices. | ||
Operational Assessment |
Assess potential for specific interventions. |
Assess consumption by target groups of potential vehicles for fortification. |
Adapted from Gillespie and Mason (1994).
It may be prudent to delay conducting in-depth assessments until pilot programmes have clearly revealed what additional information is needed for long-term planning. Disaggregated information on the location and seasonal variation of deficiencies and on the affected population groups will permit better analysis of the problem.
Further information on clinical and biochemical methods to assess the micronutrient status of populations can be obtained from FAO WHO the International Council for the Control of Iodine Deficiency Disorders (ICCIDD) the International Vitamin A Consultative Group (IVACG) the International Nutritional Anemia Consultative Group (INACG) and other organizations listed in Appendix 1.
Dietary assessment is an important step in planning food-based strategies. However simple methods to determine consumption of micronutrient-rich foods and factors that enhance or inhibit their absorption are less well-developed and less widely published than methods of clinical and biochemical assessment of micronutrient status.
Large-scale dietary assessment surveys are complicated time-consuming and expensive to conduct and analyze. Full use should be made of information from existing studies; however planners should exercise caution in making generalizations from these data and should be aware that changes in food consumption may have occurred since a study was conducted.
Dietary assessment can be simplified by focusing on nutrients of public health concern and common foods that supply them. Updated food composition tables should be used and should be specific to the region where possible. For some purposes rapid assessment methods can be used to estimate vitamin A intake. Data collection methods which estimate quantitative consumption of various vitamin A foods are often not necessary because qualitative food frequency questionnaires provide enough information to evaluate the general adequacy of vitamin A intake. (See Exhibit 3.1.)
Exhibit 3.1. Food Source of Vitamin A, Iron and Iodine Food Sources of Vitamin A: Vitamin A is present in the diet in two forms: preformed vitamin A or retinol provitamin A, primarily beta-carotene and other carotenoids which are converted to retinol in the body NOTE: Dietary fat is necessary for absorption of vitamin A, especially beta carotene. Foods rich in retinol: colostrum, breast milk, liver (chicken liver may be least costly), eggs, whole milk Tropical and subtropical plant foods rich in beta-carotene: Leafy Greens (1800 to 6000 international units per 100 grams) Fruits (1000 to 4700 international units per 100 grams) mango, Pirie and Haden varieties (Margifera indica) (darker varieties contain higher levels) passion fruit (Passiflora edulis) papaya (Carica papaya) (darker, hybrid varieties contain higher levels) poha (Physalis peraviana) avocado, Beardslee variety (Persea americana and P. drymifolia) persimmon (Ddiospyros kaki) surinam cherry (Eugenia uniflora) loquat (Eriobotyra japonica) Tubers (6400 international units per 100 grams) sweet potato (orange varieties) (Ipomoea batatas) Flowers (4800 international units per 100 grams) pumpkin (Cucurbita pepo) flower Other Plant Sources carrot (Daucus carota) ivy gourd (Coccinia cordifolia) pumpkin (Cucurbita pepo) red pepper (Capsicum frutescens) red sorrel (Hibiscus sabdariffa) red palm oil leaf protein concentrate Food Sources of Iron: Breast milk (when fed during the first 6 months of life) Haem Iron (animal foods) blood (blood sausage, blood pudding) meat, liver, fish Non-haem Iron (plant foods) seeds, legumes and products (3 to 12 milligrams per 100 grams) leafy greens (1 to 4 milligrams per 100 grams) Iodine: Breast milk from mothers with good iodine status Animal foods rich In Iodine: sea (marine) fish marine shellfish animal products, especially milk, from animals with good iodine nutrition Plant foods rich in iodine: seaweed plants from soil rich in iodine |
The seasonality of vitamin A deficiency and the availability and consumption of fats and oils necessary for vitamin A absorption should be assessed. I he diets of young children may be very low in fat; in addition children suffering from protein-energy malnutrition (PEM) may have reduced levels of the serum protein that transports vitamin A and children often have very i different vitamin A consumption patterns than adults in the family.
Dietary assessment methods for estimating consumption of retinol, carotene folic acid and other nutrients are continually being refined and improved. Information about up-to-date methods of rapid assessment of vitamin A consumption can be obtained from IVACG and Helen Keller International. (See Appendix 1.)
In assessing dietary iron intake, planners need to be aware that the bioavailability of dietary iron is more important than the amount consumed. Iron is present in adequate amounts in most diets. However, iron deficiency is common for several reasons: poor absorption, especially from plant sources (non-haem iron); high iron requirements among women during pregnancy and among growing children; and blood loss caused by menstruation, childbirth, parasitism and accidents.
Haem iron found in animal products (meat, fish, poultry, liver, blood) is better absorbed by the body. Non-haem or plant sources of iron (legumes, vegetables, cereals) are much less bioavailable. Foods that contain tannins, phytates, oxalates and certain proteins inhibit absorption of nonhaem iron. However, meat and fish, foods rich in vitamin C, and certain fermented foods all increase absorption of non-haem iron. (See Exhibit 3.2.) People with lower iron status tend to absorb the mineral better from food. For all of these reasons, assessments of dietary iron intake must take into account both bioavailability and intake of foods that inhibit or enhance iron absorption as well as status of parasitic infections.
Exhibit 3.2. Enhancers and Inhibitors of Iron and iodine Absorption Enhancers of Iron Absorption Animal foods: fish meat shellfish breast milk, when breastfeeding exclusively Vitamin C-rich foods: Breast milk (from mothers with good vitamin C status) NOTE: Vitamin C-rich foods enhance absorption of iron from plant foods. Dark green leafy and other vegetables (930 to 140 milligrams per 100 grams, although losses in cooking can be high): amaranth leaves (Amaranthus spp.) malabar nightshade (Basella spp.) beet greens (Beta vulgaris) lotus root (Nelumbium nelumbo) spinach (Spinacia oleracea) broccoli (Brassica oleracea, var. Italica) Chinese cabbage (Brassica pikinensis) head cabbage (Brassica oleracea var. capitata) cabbage (Brassica oleracea) green pepper (Capsicum annum) red pepper (Capsicum frutescens) bean sprouts (Phaseolus vulgaris) belembe or Tahitian taro (Colocasia spp.) taro leaves (Colocasia esculentum; Arum esculentum) watercress (Nasturtium officinale R. Br.) Fruits (30 to 2300 milligrams per 100 grams): guava (Psidium spp.) mango, ripe (Mangifera indica) papaya (Carica papaya) pineapple (Ananas cornosus) citrus fruits many varieties of wild fruits and berries Root crops: potatoes, sweet potatoes (may contain small but useful amounts after cooking) Fermented foods: local "sour porridge" made using lactic-acid-producing bacterial cultures fermented vegetables such as sauerkraut sourdough bread soy sauce Inhibitors of Non-haem Iron Absorption (When Consumed in the Same Meal) Tannins (found in tea, coffee, red sorghum, eggplant, legumes, many dark green leafy vegetables, and oregano), phytates (found in whole grains and high-extraction flours) and oxalates are known to reduce iron absorption in the small intestine. However, numerous interactions occur between nutrients and food components consumed in the same meal. Some of these interactions enhance absorption, whereas others inhibit absorption of non-haem iron. While it is not necessary to ban a food because it contains inhibitors, sound dietary advice can be offered to limit any negative effects. For example, people should be encouraged to drink tea between meals. Some processing techniques have a beneficial effect. Leavening reduces phytate levels, and fermented breads have little effect on iron absorption. Inhibitors of iodine Absorption Possible goitrogens: Brassica genus, including cabbage, mustard greens, radish, turnips, horseradish certain varieties of millet bitter varieties of cassava, especially if inadequately processed soybeans red skin of peanuts Generally, the people are aware of which plants contain goitrogens and have developed food-processing techniques to remove them. In some parts of Africa, cassava is steeped and fermented, which releases the cyanogenic compounds that are goitrogenic. |
Assessment of dietary iodine intake is usually not necessary because dietary intervention for iodine consists almost exclusively of fortification, almost always with salt. The dietary assessment issues to consider in designing an iodine fortification programme are described in Section 2.5, Food Fortification.
In some countries, it may be helpful to assess the role of goitrogens, which can interfere with iodine absorption. Goitrogens may be found in water, improperly processed bitter varieties of cassava, certain strains of cabbage and other vegetables, and certain cultivars of millet. (See Exhibit 3.2.) However, when diets contain adequate amounts of iodine, most goitrogens do not interfere with iodine metabolism. Furthermore, it is difficult to determine exactly which foods in any given area have goitrogenic effects. In countries where many people eat goitro-genic foods, it may be prudent to establish aboveaverage levels of iodine fortification.
Programmes that effectively address micronutrient malnutrition are based on an understanding of the factors that affect micronutrient status. Although poor dietary intake of micronutrients is often the major cause of micronutrient malnutrition, non-diet-related factors can also play an important role. Causes of malnutrition may be classified as direct or immediate, underlying or mediated by other factors, and root factors such as poverty from which other factors often stem. (See Table 3.2.)
Table 3.2. Causes of Micronutrient Deficiency Immediate n low intake of foods rich in micronutrients n low intake of substances like vitamin C that enhance absorption n high intake of factors like phytates and tannin that inhibit absorption n high incidence of measles, diarrhoea and parasitic infections n maternal deficiencies Underlying n inadequate breastfeeding practices n inadequate and/or incorrect complementary feeding practices n inadequate caring capacity: time, knowledge, etc. n low levels of family education, awareness, knowledge and motivation n intra-household maldistribution of access to food, health services and care n poor cooking, food preparation, storage, preservation and processing facilities and practices at household levels n beliefs and practices that restrict access to certain foods for some family members n poor health service and/or agricultural infrastructure n lack of institutional capacity in nutrition and/or personnel trained in the various components of micronutrient deficiency prevention programmes n low production of micronutrient-rich foods n lack of household-level gardening n insufficient marketing infrastructure for key foods n poorly developed commercial food-processing industry Basic n lack of resources to produce micronutrient-rich foods n failure to consider micronutrient needs in agriculture and health policy-making n poor economic or physical access to markets n little or no productive land n lack of access to seed and other inputs n lack of access to water for drinking, hygiene and/or irrigation n seasonality of food availability n low status of and lack of resource control by women n high prevalence of certain endemic diseases Adapted from Gillespie and Mason (1994). |
Underlying factors affecting micronutrient intake generally fall into three broad categories. Analysis of these factors in relation to specific micronutrient deficiencies may help to identify appropriate preventive measures.
n Food factors relate to household food security (year-round access to adequate amounts of safe, good-quality food for all family members).
n Health factors relate to health care and sanitation.
n Care factors relate to individual care and feeding practices, particularly among vulnerable groups such as young children.
Food restrictions and the preferences of groups vulnerable to micronutrient malnutrition, including young children and pregnant and lactating women, must always be considered when designing programmes to prevent micronutrient deficiencies. This is particularly important if communication strategies are used to affect consumption. Decision making at the household level, including time allocation and the work burden of family members, will affect the availability of food and health care (Kumar 1994). In areas where change is occurring rapidly as a result of urbanization, road construction in rural areas and the establishment of rural industries, shifts in attitudes and time allocation as well as diet are likely to occur.
In most countries, government policies on agriculture and trade greatly influence the availability and price of micronutrient-rich foods, as well as the profitability of producing, processing and marketing such foods. Reviewing such policies for their impact on micronutrient status is an important step in planning food-based strategies. In most countries where micronutrient deficiencies are a public health problem, policy changes could improve the availability of micronutrient-rich foods.
Figure

Figure

Governments should encourage the preservation and processing of excess food produced during the peak season to ensure year-round availability. This abundant mango harvest in Guinea can be enjoyed now and later. As part of a regional rural development strategy in the country, families are encouraged to process mangoes as jam (shown here), juice, and dried fruit for use in the off-season.
Policies relating to export crops and staple cereal foods may need to be reassessed if cereals can potentially be used as fortification vehicles or if increased local consumption of certain exported foods is considered desirable. Regulations which prohibit gardening in urban areas or restrict the marketing of fresh foods may have an impact on the availability of micronutrient-rich foods.
Governments should be encouraged to adopt policies that promote the availability of micronutrient-rich foods. For example, horticultural programmes extension networks can incorporate strategies to increase the production, distribution and marketing of perishable products such as fruits and vegetables. The preservation and processing of excess food produced during the peak season encourages the production of low-cost micronutrient-rich foods and ensures yearround availability of these foods. The development of local food preservation and processing facilities can be encouraged, with the involvement of both the private sector and local producer and consumer cooperatives.
Figure

An international project assisted the Zambian government to bring about reform In the marketing of maize and other staples, with a view to achieving cost-efficient marketing and, in turn, improved food security. This dally open-air market In Kabwe caters to the food needs of the local population.
National agriculture planning strategies have been shown to have an impact on micronutrient status (FAO 1996, Mansour et al. 1994, Ngu et al. 1995). Approaches taken include crop diversification to promote micronutrient-rich minor crops; agroforestry projects; promotion of traditional and wild foods; and encouragement of horticulture and small, family-based production and consumption units.
Price is a major determinant of consumer choice to purchase micronutrient- rich foods. Inexpensive fruits and vegetables, including green leaves, are the primary sources of vitamins A and C in many people's diets. In the Philippines, dietary intake of these vitamins varied directly with the price of green leafy vegetables (Bouts 1991).
Nutrition education and increased home production are more likely to increase consumption of foods rich in vitamins A and C than of iron-rich foods. Sources of dietary iron are less subject to seasonal fluctuations in availability and price. Consumption of foods that provide bioavailable haem iron and retinol usually increases rapidly as income rises because higher earnings lead to more purchases of animal food.
An initial assessment should review how micronutrient-rich foods are processed, stored and marketed. This review should include an examination of how well developed the infrastructure is (particularly roads and commercial markets). The feasibility of increasing the availability of small animals and livestock should also be reviewed.
Improving market efficiency may allow food prices to fall for consumers while increasing growers' profits. In some countries, the change to an open-market system may disrupt traditional food availability but may also present opportunities for improved food marketing. In other countries, the establishment of cooperatives to eliminate the middleman may contribute to lower consumer food prices without decreasing producer earnings.
Programme planners should be aware that cultural preferences for certain foods can affect micronutrient status, despite (or independent of) education efforts. In most cultures, some micronutrient-rich foods, such as animal products and certain fruits and vegetables, are prized and sought after by the population. However, poor and vulnerable groups may have limited access to these foods or they may prefer to sell them.
Price information may be readily available for foods such as cereals, pulses and meat. However, in some regions, wild fruits, vegetables and leaves make valuable seasonal contributions to many people's diets. Because these foods may not be sold in markets, information about their prices may not be readily available. Planners should endeavour to assess the availability of these foods and determine how the consumption of these foods is influenced by price changes and income levels and the extent to which prices of these foods vary with increases or decreases in supply. Processed foods and potential vehicles for food fortification should be examined in the same way.
Finally, an initial assessment should review relevant food laws and regulations. Factors related to import and export policies, as well as to informal border trade, can have a great impact not only on diets and food availability but also on the outcome of food pricing and subsidization policies, such as those related to salt and other fortified foods. (See Section 2.5, Food Fortification.)
Once the nature and causes of a micronutrient malnutrition problem have been defined, it is important to review existing financial and human resources to determine the magnitude of additional resources needed to solve the problem. The term "resources" should be interpreted broadly to include laws; government policies; agriculture, health, education and communication programmes and projects; and technical or professional capacity at both the national and the community levels. The feasibility of various interventions will be determined to some extent by the level of funding that can be committed to a micronutrient programme.
Personnel training needs must be considered early in the planning process. Staff at existing research and training institutions may or may not have training and experience that is relevant to the implementation of a micronutrient programme. If a large programme is to be implemented, training of several levels of personnel may be required. Because this training "cascade" (in which staff at each level are trained to instruct the staff they supervise) can take some time to complete, it is important that the process begin early.
Figure

Government policies on agriculture and trade greatly Influence the availability end price of micronutrient-rich foods. These workers are sorting and packing freshly harvested tomatoes on a cooperative plantation in Honduras. This abundant harvest was made possible by a comprehensive action to improve the irrigation system in Honduras.
In addition to teaching the skills required to implement a programme, it is also important to develop the skills necessary to conduct continuous programme monitoring and evaluation. Appropriate skills include the collection, management, analysis and reporting of data. Monitoring and evaluation methods and indicators must be selected early in the planning process and training must be tailored accordingly.
When the use of communication strategies is being considered, planners should be aware of which mass media vehicles (e.g., newspapers, magazines, radio, television and cinema) reach which segments of the population. It is also useful to understand the structure and expertise of the local advertising industry and, in particular, to know whether the industry has previous experience in social marketing techniques. The communication skills of staff within health education departments and agricultural extension services will also contribute to the successful implementation of communication strategies.
Programmes to increase the availability and consumption of micronutrient-rich foods may not have the expected impact on micronutrient status if preexisting health factors have not been reviewed and taken into consideration. Micronutrient status is influenced by the body's requirements for the micronutrient as well as by intake and absorption. Nutrient requirements vary depending on physical growth rates, activity levels and general health status. In women, reproductive status (i.e., whether they are pregnant or lactating) is also an important factor. Parasitic infections, diarrhoea, protein-energy malnutrition and other serious illnesses common among young children in the developing world can interfere with nutrient absorption and utilization.
Reports from ministries of health, UNICEF Country Situation Analyses and the medical literature can usually provide data on the prevalence of parasitic infections and other diseases, as well as on breastfeeding rates. In addition to reviewing the health status of the population, planners should obtain information about existing public health programmes to improve water availability, quality and sanitation; provide vaccinations and oral rehydration therapy; and combat respiratory infections, tuberculosis and malaria and other parasitic diseases.
Information concerning agricultural production and services and food availability and distribution systems, as well as the existence of central food and agricultural planning mechanisms, is key to planning food-based strategies to prevent micronutrient deficiencies. Seasonality and regional variations in the production and availability of foods are important issues to consider when attempting to ensure the year-round availability of micronutrient-rich foods.
Local efforts through agricultural extension services to promote the production and consumption of micronutrient-rich foods are fundamental to ensuring the year-round availability of such foods. The agricultural sector can promote increased production and availability of micronutrient-rich foods through research, plant breeding and crop selection. Infrastructure for the processing, preservation, transportation, distribution and marketing of micronutrient-rich foods is also important. Statistics about production and year-round market prices provide an indication of the availability of micronutrient-rich foods.
Although the three major micronutrient deficiencies have many different causes and potential solutions, opportunities exist to coordinate micronutrient deficiency control programmes. Groups vulnerable to each deficiency overlap substantially, although not completely. In certain circumstances, assessment and surveillance components can be coordinated. Programmes targeting different deficiencies can hold joint training sessions. There may also be opportunities for combined information, education and communication efforts.
The advantages of programme coordination include:
n reductions in costly duplication (Trowbridge et al. 1993),
n avoidance of unconstructive competition for funding (for example, joint grant applications may increase the likelihood of obtaining funding for all programmes), and
n an increased likelihood of reaching policy makers with effective messages.
An important advantage of food-based strategies is that foods provide many micronutrients simultaneously. Physiological interactions between vitamin A and iron suggest that a combined approach to overcoming deficiencies in these micronutrients could be beneficial. For example, programmes that promote increased consumption of vegetables to overcome vitamin A deficiency may harm iron status if the selected vegetables are high in tannins. A combined approach could avoid this problem. Gardening projects and communication programmes usually need make only small adjustments to make useful contributions to both vitamin A and iron deficiency.
Multiple fortification (for example, the production of specialty foods such as soft drinks and cookies fortified with several micronutrients) may be possible in the future. However, some technical issues involved in multiple fortification are still unresolved. The advantages and disadvantages of this approach need to be carefully considered.
Fundamental social policy and investment decisions can have important indirect effects on micronutrient availability. Frequently, however, such decisions are not made with concerns about micronutrient nutrition in mind.
n Improved access to water will increase opportunities to grow fresh fruits and vegetables that require irrigation.
n The building of new roads will lower the cost of getting micronutrient-rich produce to market.
n Increased electrical generating capacity may lower the cost of food processing.
n Increased investment in soil conservation and flood control may reduce the loss of iodine from soil.
n Clean water and sanitation projects may reduce blood loss caused by parasite infestation.
n Increased levels of female education, research in the development and marketing of inexpensive labor-saving devices for tasks typically performed by women, and improved access to child care can enable women to improve their children's food intake, thereby improving the children's micronutrient status.
n Improved university-level science education will provide the expertise needed to make many of these advances.
Other changes that can indirectly affect micronutrient availability include improvements in the small-scale and home gardening component of horticultural training for extension workers and the addition of an up-to-date micronutrient component to the training curricula of teachers, home economists and medical and health workers. Experience suggests that raising awareness among people in the health and education sectors of the adverse effects of micronutrient deficiencies can facilitate positive changes.
Difficult decisions must be taken on whether to invest effort and resources in marginally influencing larger societal processes or whether the promotion of new policies and activities which are specifically aimed at improving micronutrient nutrition is a better investment. In general, indirect approaches should be employed opportunistically rather than being a substantial component of the planning of food-based strategies.
Micronutrient deficiencies will decline as equitable development policies succeed in reducing poverty. However, the decline is unlikely to occur as quickly as protein-energy deficiency declines. Increased income leads to increased intake of fat and protein, but not necessarily micronutrients. There is no specific hunger mechanism for them. Breastfeeding rates may decline with increased income. In addition, consumption of many micronutrient-rich foods is influenced less by economic factors than by seasonality, market infrastructure and education. Micronutrient projects can be integrated into larger programmes. For example, agricultural, educational and health planners may be willing to add micronutrient components to existing broadbased programmes in their sector.
Agricultural planning is already beginning to change in ways that will contribute to improved micronutrient status, for example, through increased attention to small family production/ consumption units and to horticulture. Relevant approaches promoted by FAO include crop diversification, planting of minor crops, agroforestry (including the "Forests, Trees and People" initiative) and promotion of traditional and wild foods.
Relevant health sector programmes include the blindness prevention programme with vitamin A deficiency control components. The Safe Motherhood Initiative directs attention to anaemia during pregnancy. Some educational planners are focusing attention on interventions to reduce iron and iodine deficiencies in schoolchildren because of the adverse effects of these deficiencies on children's active learning capacity.
The diets consumed by most people in the world are nearly adequate in most micronutrients. Therefore, a key step in designing a food-based strategy to prevent micronutrient deficiencies is to determine what people are already eating and how dietary patterns are changing. Many programmes to promote food-based strategies promote new ways of storing, processing or preparing traditional foods or introduce new micronutrient-rich foods as crops or components of the diet.
For example, breastfeeding programmes in most countries concentrate initially on protecting and supporting traditional breastfeeding practices before promoting breastfeeding among non-breastfeeding women. If consumption of micronutrient-rich foods such as green leafy vegetables is low because these foods have low status in the community, the use of high-status mass media or famous personalities to promote these foods may increase both their status and their consumption. Such campaigns must be accompanied by efforts to ensure an adequate supply at an affordable price.
Integrating micronutrient components into existing health, agricultural and nutrition education policies and programmes is another way to build on what already exists. Minor changes in or additions to these policies and programmes may greatly increase their impact with minimal additional effort and cost.
When large development programmes are initiated, a component should be included to protect the population from both micronutrient deficiencies and proteinenergy malnutrition during the transition period. In Indonesia, for example, people living in villages that were moving from traditional living patterns towards a more urban living pattern were found to have the highest rates of micronutrient deficiency (Drake et al. 1993).
Programmes designed only to increase production of micronutrient-rich foods are unlikely to eliminate micronutrient deficiencies. Without nutrition education, increased production may not lead to increased consumption among vulnerable groups. Conversely, communication strategies that increase demand for a food while supply remains constant may result in an increase in the price of the food. This phenomenon has been documented in the cases of carrots in Nepal and green leafy vegetables in the Philippines. In the short term, promoting only increased consumption may harm the micronutrient status of poorer groups by reducing the amount of food they can afford to consume.
Thus, the most successful approach to increasing consumption of micronutrient-rich foods is likely to be a combined strategy that addresses both increased production (supply) and increased consumption (demand) and also meets the needs of special groups such as children and women of childbearing age.
Many types of expertise are required to develop and implement a broad-based strategy to eliminate micronutrient deficiencies. The involvement of many different organizations, all of which share responsibility for a programme, can significantly slow the pace of development and implementation. Intersectoral groups can help by ensuring that at least one representative of each involved agency understands the issues involved, has had an opportunity to uphold the agency's interests and ensures that it follows up on its responsibilities.
The hierarchical nature of government agencies, with senior officials the only ones empowered to make decisions or make statements on behalf of the agency yet rarely having time to become involved in issues perceived as being of marginal importance, can be a major constraint on collaborative efforts. The success of intersectoral groups depends on wise appointments and the delegation of authority to active and interested junior representatives. The following principles will facilitate the development of effective intersectoral collaborations:
n Only a core of key affected agencies and ministries should be invited to appoint standing members to the intersectoral group. Any absence from meetings should be followed up to ensure that all intersectoral group members remain involved.
n Meeting agendas should be planned in advance. Important decisions should not be made at meetings to which key authorities have not been invited. (If intersectoral groups want to be taken seriously, they must show respect for each member's specialized area of interest.)
n Other agencies and ministries should be invited to appoint ex officio or ad hoc members of the group. Complete minutes should be taken at all meetings and sent to all participants. Ad hoc members should be invited only to meetings that directly affect them, and then non-attendance should be followed up.
n One agency must have a budget line that allows it to use personnel and stationery for the group's work and, if possible, cover travel and subsistence costs for other group members. This is especially important if nationwide participation of the intersectoral group is desired.
Representatives from key authorities in the health, agriculture and educational sectors should be permanent members of micronutrient intersectoral groups. Authorities dealing with industry, trade and possibly mining (for salt) should be included when fortification is discussed. Authorities dealing with laws and food regulations will need to be involved to ensure compliance. Authorities dealing with children, youth and women may need to be involved when the needs of and plans for those special groups are discussed. Non-governmental organisations can provide valuable practical advice regarding community participation.
Intersectoral groups should invite participation by and explore opportunities for cooperation with the food industry. Industry representatives should always be involved in decisions on issues that directly affect their interests. Raising the industry's awareness of the importance of overcoming micronutrient deficiencies may motivate food manufacturers to devise new ways of improving the micronutrient content of their products.
Success will greatly depend on advocacy to obtain both community acceptance of and political support for programmes. When communities are directly involved in assessment, analysis and action discussions, they will be more likely to accept a strategy which they perceive to be aimed at solving a problem, even if it adds to their workload. Exhibit 3.3 describes successful coordinated approaches to the control of micronutrient deficiencies.
Exhibit 3.3. Coordinated Approaches to Micronutrient Deficiency Control Niger: The Ministry of Agriculture, in collaboration with the Ministry of Health and Education, implemented a successful 2-year pilot project which demonstrated the benefits of integrating agricultural-and health-sector approaches to the control of vitamin A deficiency. Project goals were to increase production and promote consumption of locally available vitamin A-rich foods. FAO and the Vitamin A Field Support Project (sponsored by the U.S. Agency for International Development) provided technical assistance and support for nutrition education and communication, horticultural techniques and food preservation as well as monitoring and evaluation. The project demonstrated that a strong nutrition education component promoted the consumption of underutilized sources of vitamin A, such as traditional green leaves and liver. Some wild plants were successfully cultivated. Seasonal shortages were addressed through food preservation techniques such as solar drying. Improved vitamin A status was documented even among children in the project area, a finding that was not observed in the non-project area (Mansour et al. 1994). Tanzania: Although no national micronutrient surveys have been conducted, scattered surveys showed the existence of deficiencies of vitamin A, iron and iodine. National intersectoral committees were established for each deficiency. Each committee included in its membership all relevant national authorities. The Tanzania Food and Nutrition Centre (TFNC) acted as secretariat. A national workshop was held for each deficiency, in which experienced field staff from around the country, as well as local and international experts, were invited to participate. Recommendations from the workshops were used to design 5-year plans which combined diet-based approaches with shortterm supplementation targeted to the most severely affected groups. All the plans included information, education and communication components. Fortification is being explored and iodisation of salt is already occurring. The key to progress so far (which has occurred in spite of the country's economic problems) is the gradual evolution of a strong national nutrition institution (TFNC), which has an inclusive way of working and sharing resources with the collaborating partners needed. Vietnam: From 1991 to 1993, FAO implemented a vitamin A deficiency control pilot project in four Vietnamese communes, using a long-term, preventive, multi-sectoral strategy. The major interventions were nutrition education for pregnant women and women with children under 5 and promotion of the production of vitamin A-rich foods in home gardens. A network of community volunteer educators ensured service delivery at the grass roots level. Baseline and follow-up surveys measured changes in mothers' knowledge and child-feeding practices, food production and use, food consumption patterns and nutritional status. Over 2 years, mothers' knowledge scores increased by 26% and the number of mothers who used vegetables in complementary foods increased 32%. Home production of vegetables increased from 41 to 233 g per person per day; most produce was consumed at home. Both overall food intake and vegetable consumption among children under 5 increased. Xerophthalmia prevalence decreased significantly. The project had a positive impact on health, nutrition and household food security in the target communes (Ngu et al. 1995). |
![]()
![]()
![]()
![]()